That's a Wrap: 'Sine Die' at the 2026 General Assembly. Here's where EM landed.
The 2026 Virginia General Assembly has officially adjourned “Sine Die” — a Latin term meaning “without a day,” signaling the formal end of the legislative session. Gov. Abigail Spanberger has until 11:59 p.m. on Monday, April 13 to sign, veto, or amend legislation, and the General Assembly will reconvene on April 22 to consider her actions.
Emergency physicians were closely watching several major policy debates, including a proposal to dramatically raise Virginia’s medical malpractice cap, legislation affecting physician assistant practice authority, new restrictions on healthcare non-compete agreements, and ongoing efforts to address workplace violence and behavioral health challenges in the Commonwealth’s healthcare system.

Aimee Perron Seibert, VACEP lobbyist
While the most sweeping malpractice proposal ultimately shifted to a data-collection approach for now, the session still produced several changes that will affect physicians and hospitals across Virginia.
“This was a session where a lot of big issues were on the table for healthcare,” said VACEP lobbyist Aimee Perron Seibert. “In the end, emergency medicine avoided some of the most concerning proposals, and we were able to improve several bills along the way. But many of these issues — especially medical malpractice — are far from settled and will continue to be major conversations moving forward.”
Here’s a look at the legislation and policy developments in Virginia EM.
Medical malpractice debate shifts to data collection
In one of the most closely watched late developments of the session, lawmakers ultimately backed away from a proposal that would have immediately raised Virginia’s medical malpractice cap from $2.7 million to $6 million.

Lawmakers heard from medical and specialty groups like VACEP, which helped to stop a proposal that would have immediately increased Virginia’s medical malpractice cap to $6 million. The issue continues but is being studied.
Instead, negotiators substituted new language into the conference report for Senate Bill 536 that directs insurers and self-insured hospitals to collect detailed data on malpractice claims, payouts, and how often cases approach or exceed the current cap.
The information will be reported to the state in September and is expected to inform continued negotiations over the future of Virginia’s medical malpractice system.
While the cap increase proposal has been paused for now, the debate is far from over. Physicians, hospitals, trial attorneys, and lawmakers are expected to continue discussions starting this spring as policymakers review the new data and consider possible changes in future sessions.
BILLS VACEP SUPPORTED
KeepING patients who lack consent in the ER when they have a critical medical need | HB309 (Hope)
Status: Passed and awaiting Governor’s signature
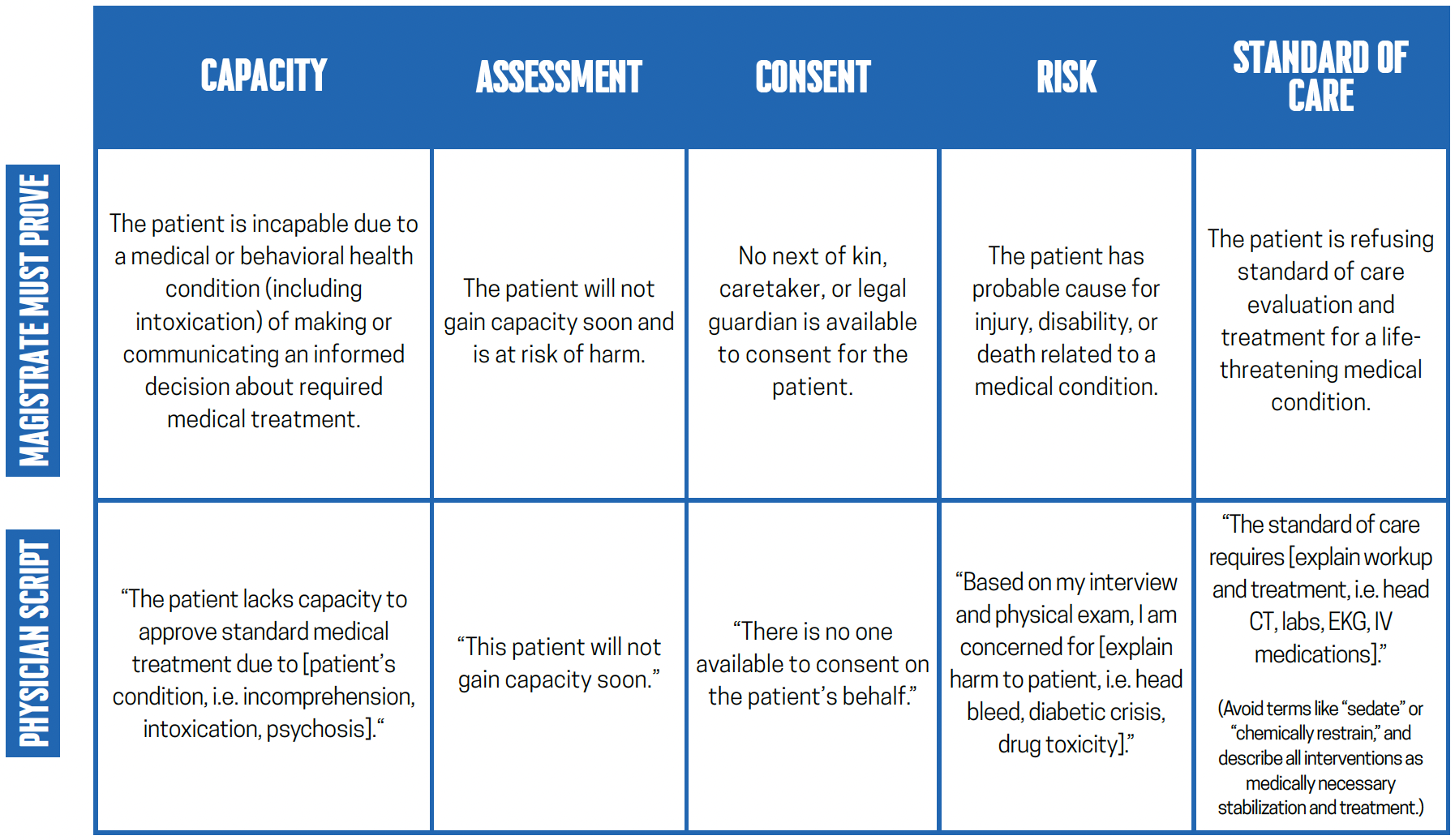
Under current Virginia law, physicians must obtain a court- or magistrate-issued medical Temporary Detention Order (TDO) to treat patients who cannot consent to care due to conditions such as intoxication, delirium, or hypoxia. However, the law does not clearly define who has custody of a patient during the critical window between arrival in the ER and issuance of that order.
Introduced by VACEP, the bill clarifies that while a medical TDO is being sought, a patient who lacks capacity is to remain in the custody of the hospital, allowing security staff to prevent the patient from leaving for a limited period. The bill does not expand detention authority, extend the duration of a TDO, or create new standards for involuntary treatment, and preserves existing liability protections for clinicians acting in good faith.
VACEP leaders volunteer hundreds of hours each year to advocate and track legislation. We also give to lawmakers to ensure we elect pro-emergency medicine candidates who support the patients under our care. Give today to the Emergency Medicine Political Action Committee in Virginia (EMPAC-VA).

Emergency physicians with Mark Downey, M.D. at EM Advocacy Day. Downey, whose district covers York County and surrounding areas, is the only doctor in the General Assembly after winning election in November.
Improving the review and disciplinary process for Board of Medicine complaints | HB1139 (Downey)
Status: Passed and awaiting Governor’s signature.
Introduced by VACEP, the bill modernizes the makeup of Virginia’s Board of Medicine.
Currently, the board is the only health regulatory board in the Commonwealth required by statute to appoint physician members based on congressional districts rather than clinical expertise. That structure limits specialty representation on a board that primarily handles disciplinary complaints and standard-of-care reviews.
The change will remove the geographic requirement and allow appointments based on medical licensure, improving access to specialty expertise without altering the board’s authority or mission.
Physician non-compete restrictions advance | HB627 (Helmer) & SB128 (VanValkenburg)
Status: Passed and awaiting Governor’s signature.
The bills limit the ability of employers to enforce non-compete agreements against physicians and other clinicians, a change supporters say could help address workforce shortages and allow physicians to continue caring for patients in their communities.
Virginia already faces a shortage of nearly 4,000 doctors. Limiting where clinicians can practice only exacerbates delays in specialty coverage and transfers — problems felt acutely in emergency departments.

Virginia emergency physicians on the steps of the General Assembly Building at EM Advocacy Day on January 28 in Richmond. There, they expressed support and voiced opposition for various pieces of legislation under consideration.
Budget language revisits psychologist prescribing debate
Language included in the Senate budget would require the Department of Health Professions to study the qualifications that would be needed if psychologists were ever allowed to prescribe medications.
A similar study conducted last year ended in a stalemate, but participants did agree psychologists did not have the right education or training to gain prescribing authority. The proposal is still tied to the ongoing budget negotiations and may change before the final budget is adopted.
BILLS VACEP OPPOSED
Doctors as petitioners for “substantial risk orders” | HB901 (Sullivan)
Legislation expanding who may petition courts for a firearm substantial risk order passed this year.
The law allows healthcare professionals to seek such orders but does not require them to do so. Physicians may still choose to work through law enforcement if they believe a substantial risk order is warranted.
Workplace violence reporting clarified | HB1489 (TRAN)
Lawmakers passed a follow-up measure clarifying last year’s legislation requiring hospitals to internally report incidents or threats of workplace violence.
The new bill expands and clarifies reporting requirements and definitions as hospitals continue implementing the statewide reporting framework.
Narrow psychiatric emergency department provision | HB1318 (WILLETT)
Another bill addressed a unique situation involving Riverside Health System’s psychiatric emergency department in Hampton.
The legislation allows that facility to continue operating without a physician physically on-site under specific conditions, including transfer agreements with nearby hospitals and other staffing safeguards. The provision is narrowly written and applies only to that facility. Virginia law, in effect as of July 2025, requires that all emergency departments have a physician on-site 24/7, so the bill applies only to this one psychiatric ED — the first of its kind in the Commonwealth.
Lawmakers noted that the psychiatric emergency department has treated thousands of patients and helped reduce pressure on nearby emergency departments.
Changes to physician assistant practice law | HB746 (Henson)
Lawmakers approved legislation to create a framework for physician assistants to practice without a formal practice agreement — after meeting certain experience thresholds, including practicing with a physician in their specific specialty for three years.
During negotiations, physician groups including VACEP successfully pushed for several guardrails, including clearer requirements for physician attestations confirming a PA’s experience and language clarifying that the required experience must occur within the PA’s clinical specialty.
Additional provisions were also added to address how the law interacts with the interstate physician assistant licensure compact.
While emergency physicians continue to emphasize physician-led care as the gold standard, the amendments removed several concerns that had prompted earlier opposition to the bill.
“These safeguards are necessary to protect patient safety, ensure appropriate training and supervision, and prevent clinicians from moving into unfamiliar specialties without sufficient physician involvement,” said Jesse Spangler, MD, FACEP, VACEP’s immediate past-president.

VACEP president Joran Sequeira, MD and immediate past-president Jesse Spangler, MD at VACEP’s EM Advocacy Day.